CAPP Component 1: Access to Sexual Health Care
CAPP providers are charged with working in their communities to remove the barriers that youth experience when they need family planning and sexual health care. What will that look like in your community?
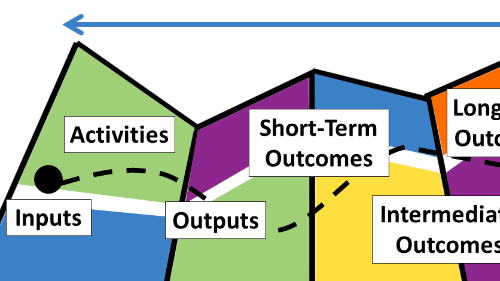
To help you get started with this objective of CAPP Component 1, we've taken a logic model approach. Below we've largely drawn from the current CAPP RFA, the guiding document from the New York State Department of Health (NYSDOH), as well as the CAPP work plan, to suggest how you might plan for this required task.
We strongly recommend that you involve young people from the communities you aim to serve in this planning process.
Planning Process: Improving Access to Services
What priority population of young people are you trying to reach? In the CAPP initiative, priority populations may include youth who are from marginalized adolescent populations, including but not limited to youth who:
- are from racial and ethnic minorities
- are from socioeconomically disadvantaged communities
- are living in foster care
- identify as lesbian, gay, bisexual, transgender, and/or questioning
- have special health care needs (including cognitive learning delays, autism spectrum)
- are homeless
- are involved in the juvenile justice system
Which of these groups do you intend to reach with your project?
The CAPP initiative aims to prevent adolescent pregnancy, sexually transmitted infections, and HIV. The initiative also aims to advance health equity in communities where program impact will be greatest. Specifically where health care access is concerned, a CAPP project's goal is to:
- Increase the number of adolescents in priority communities who receive family planning and preventive sexual health care services
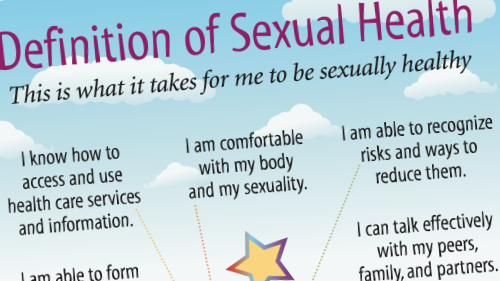
What outcomes for youth do we want to see?
If we are to achieve this goal, what competencies, attitudes, and knowledge do we want young people to develop? Examples include:
- Increased knowledge of when, where, and how to access family planning and sexual health services
- Increased confidence in family planning and sexual health services, including trust that services are confidential
- Decreased stigma around caring for one's reproductive and sexual health
- Increased self-efficacy (belief in one's capacity to accomplish a specific task or goal) for accessing services
- Improved family communication around reproductive and sexual health care
What are the barriers to these outcomes?
What stands in the way of greater access to reproductive and sexual health care services?
Check the Research
Existing research and your own previous experience with practice are good places to start (but not end) this inquiry. What does research tell us about breaking down barriers to sexual health care? Reviews of research literature have identified the following potential barriers and more [1, 2, 3]:
- Internalized stigma leading to a need to hide one's sexuality; fear of reputational damage; fear of being judged by health care providers, peers, others in community; internalized stigma leading to lack of self-love and self-care
- Power imbalances between partners; partner violence; reproductive coercion; subscribing to rigid gender roles and double standards
- Trust that partner is monogamous; desire to be more intimate with main partner (leading to condomless sex); fear of rejection; discomfort talking about safer sex with partner
- Fear of parent finding out; fear of having one's business known; lack of confidence in confidentiality of services
- Inability to talk with parents/family about prevention; parental discomfort with having conversations about sex and sexuality
- Peer norms that discourage prevention
- Lack of transportation
- Lack of access to low-cost, confidential health care; lack of trust in health care providers; inability to find a health care provider who speaks their language, is of the same race, can relate to them;
- Lack of youth-friendly services
- Invisibility within health care system (e.g., LGBTQ teens); lack of meaningful conversations with health care provider; false assumptions by provider
- Not knowing where to go for services; misinformation about services; not knowing what to expect, fear of the first visit
- Misinformation about condoms, contraception
- Lack of knowledge about sexual health and prevention; feeling sexual health information/education is not relevant or real; selecting one strategy (e.g. testing) instead of using multiple strategies (e.g. testing and using condoms); misunderstanding risk
- Dangerous and chaotic environments
- Racism, homophobia, transphobia, sexism, community and police violence leading to hopelessness; fatalism that leads to belief that preventive measures are pointless
- Lack of attractive developmental opportunities available
- Desire to have a baby or ambivalence about pregnancy
- Fear of positive test results
Learn what is happening locally
Existing research is not a substitute for understanding the local context and hearing from young people you hope to serve. Identifying local barriers that affect the priority population is a required activity for the CAPP grant.
- Conduct community assessments to uncover specific factors and barriers that impede youth access to confidential sexual health and family planning services
There are a variety of ways you could fulfill this requirement. For example, you may wish to conduct focus groups with young people; involve youth in the planning process; and/or interview service providers, youth from the priority population, and parents/caregivers.
Which activities and strategies might help break down these barriers?
Once you have identified barriers that affect the population you wish to reach, it's time to consider how you can be most effective. Not every barrier is amenable to change by your organization. Where are you most likely to be able to make a difference for the youth you support?
Potential strategies/activities
For example, to increase awareness of family planning and sexual health services, activities could:
- Reach youth with sexual health information through text messaging, digital media videos, public service announcements, social media campaigns, websites, mobile apps
- Provide youth information about local family planning and sexual health services, including the Family Planning Benefit Program
- Conduct in-person or web-based clinic tours
- Address concerns about the confidentiality of services
Work with Youth
To increase your effectiveness, work with youth in the priority population to identify barriers to services as well as strategies to address those barriers.
What resources do we have to support the effort?
Often labeled "inputs" in logic models, these resources include our organizational capacity, staff expertise, resources, and community partners that make it possible for us to offer this programming.
Typically labeled "outputs" in logic models, these actions, products, or measurements allow us to take stock of our efforts to move toward our goals. Here we list measurable actions such as number of activities to address barriers to access, number of participants, products developed, referrals completed, community partner contacts, etc. Report these outputs in your bi-annual report.
Your ACT for Youth support team is available to help you plan for impact!
References
- Bender, S. S., & Fulbright, Y. K. (2013). Content analysis: A review of perceived barriers to sexual and reproductive health services by young people. The European Journal of Contraception & Reproductive Health Care, 18(3), 159-167.
- Garrido, M., Sufrinko, N., Max, J., & Cortes, N. (2018). Where youth live, learn, and play matters: Tackling the social determinants of health in adolescent sexual and reproductive health. American Journal of Sexuality Education, 13(3), 269-282.
- Schantz, K., Amankwaa, V., & Lam, B. (2020). What are they thinking? Social and personal pressures on young people's sexual decisions: Review of qualitative literature. ACT for Youth Center for Community Action.
actforyouth.net/resources/ashrp/sti-qualitative-lit-review-2020.pdf